
Clinical characteristics of cystic biliary atresia
Keywords:
Cystic biliary atresia, jaundice, Kasai operationAbstract
Background: Cystic biliary atresia (BA) is a unique form of BA that can be mistaken for a choledochal cyst. This study reviews the clinical characteristics of cystic BA to better understand its nature.
Objective: To characterize cystic biliary atresia in terms of clinical presentation, imaging findings, and surgical outcomes, and to highlight key features that aid in differentiating it from choledochal cysts.
Methods: We retrospectively reviewed the charts of all infants diagnosed with cystic BA from January 2005 to December 2019. The diagnosis of BA was confirmed in all cases by intraoperative cholangiography. Moreover, clinical data, pre-operative laboratory and imaging, intraoperative findings, and postoperative outcome were recorded, and data were expressed as mean ± standard deviation.
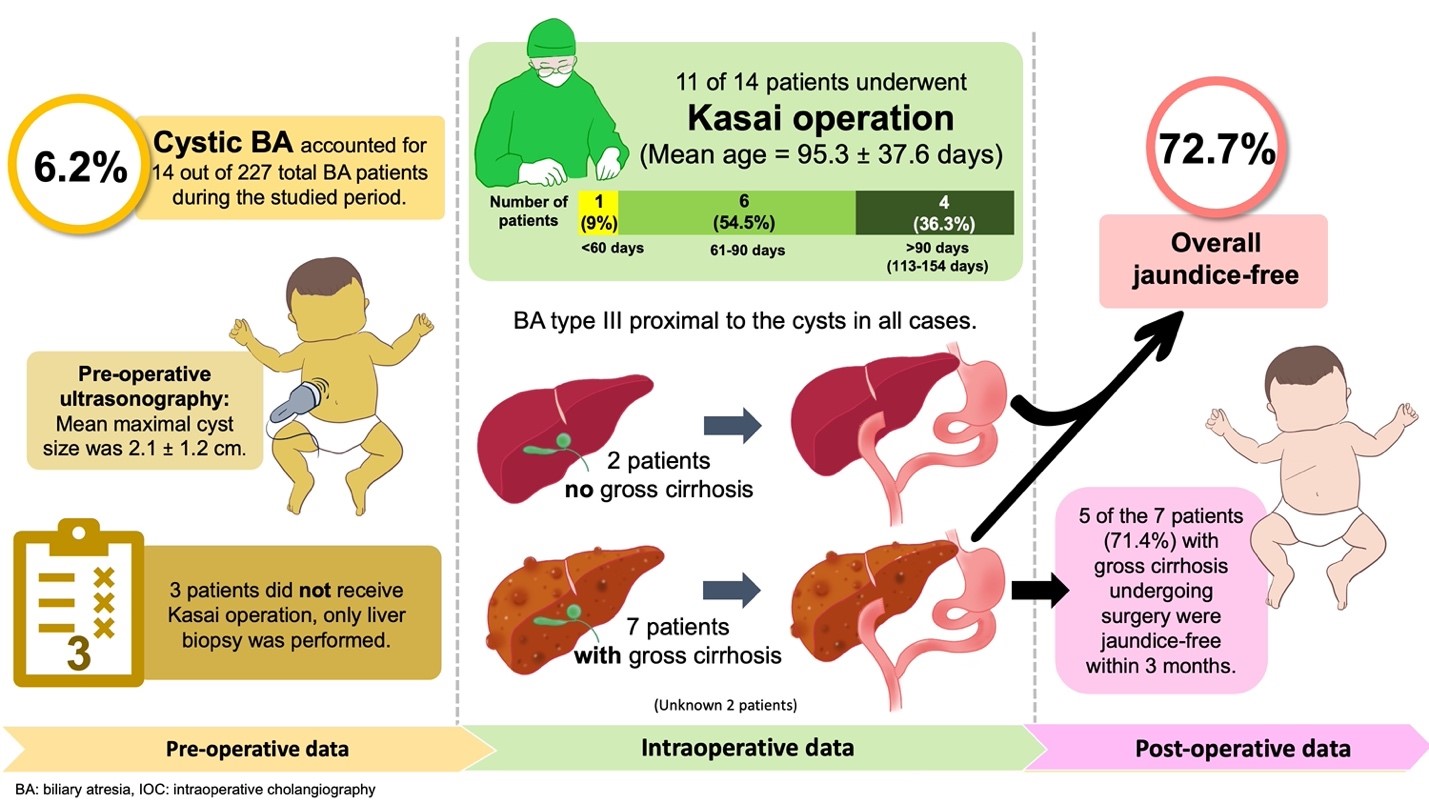
Results: Out of the 227 patients with BA, there were 14 patients with cystic BA (6.2%) during the studied period. The mean pre-operative ultrasound size at the maximal part of the cyst was 2.1 ± 1.2 cm, and 11 of 14 patients underwent a Kasai operation. The mean age at the time of Kasai operation was 95.3 ± 37.6 days, and only 1 in 11 patients (9.0%) underwent a Kasai operation before 60 days. Moreover, 6 patients (54.5%) underwent a Kasai operation at 61–90 days, whereas 4 patients (36.3%) underwent a Kasai operation at 113– 154 days. Intraoperative findings revealed BA type III proximal to the cysts in all cases. Based on the surgeons’ decision, 3 patients did not receive a Kasai operation, and only a liver biopsy was performed. After the Kasai operation, 8 out of 11 patients (72.7%) experienced no jaundice within 3 months. In addition, gross cirrhosis was recorded by the surgeons in 9 patients, and of these patients, 7 underwent a Kasai operation. Interestingly, 5 of the 7 patients with gross cirrhosis undergoing surgery (71.4%) were jaundice-free within 3 months. Briefly, an overall jaundice-free state was achieved in 72.7% of patients with cystic BA who underwent a Kasai operation. In addition, 71.4% of patients with cystic BA and gross cirrhosis undergoing surgery were jaundice-free.
Conclusion: Cystic BA is a rare pathology that needs to be distinguished from choledochal cysts in neonates. Awareness of the existence of cystic BA may facilitate the diagnosis and dissection around the porta hepatis area during the Kasai operation. This may increase the chance of better results for the patients. Even in the presence of gross cirrhosis, the Kasai procedure may still be considered to provide an opportunity for bile drainage.
Downloads
References
Sookpotarom P, Vejchapipat P. Non-correctable biliary atresia with large extrahepatic cyst: a report of two cases. Eur J Pediatr Surg 2007;17:295-7.
https://doi.org/10.1055/s-2007-965537
Schooler GR, Mavis A. Cystic biliary atresia: A distinct clinical entity that may mimic choledochal cyst. Radiol Case Rep 2018;13:415-8.
https://doi.org/10.1016/j.radcr.2018.01.025
Yoon HM, Suh CH, Kim JR, Lee JS, Jung AY, Cho YA. Diagnostic performance of sonographic features in patients with biliary atresia: A systematic review and meta-analysis. J Ultrasound Med 2017;36:2027-38.
https://doi.org/10.1002/jum.14234
Puglia EBMD, Daltro PAN, Werner Junior H, Barreto MM, Francisco FAF, Alves Junior SF, et al. Ultrasound findings for the diagnosis of biliary atresia in neonates. Radiol Bras 2025;58:e20240102.
https://doi.org/10.1590/0100-3984.2024.0102
Napolitano M, Franchi-Abella S, Damasio MB, Augdal TA, Avni FE, Bruno C, et al. Practical approach to imaging diagnosis of biliary atresia, Part 1: prenatal ultrasound and magnetic resonance imaging, and postnatal ultrasound. Pediatr Radiol 2021;51:314-31.
https://doi.org/10.1007/s00247-020-04840-9
Ho A, Sacks MA, Sapra A, Khan FA. The Utility of gallbladder absence on ultrasound for children with biliary atresia. Front Pediatr 2021;9:685268.
https://doi.org/10.3389/fped.2021.685268
Lobeck IN, Sheridan R, Lovell M, Dupree P, Tiao GM, Bove KE. Cystic biliary atresia and choledochal cysts are distinct histopathologic entities. Am J Surg Pathol 2017;41:354-64.
https://doi.org/10.1097/PAS.0000000000000805
Lal R, Prasad DK, Krishna P, Sikora SS, Poddar U, Yachha SK, et al. Biliary atresia with a "cyst at porta": management and outcome as per the cholangiographic anatomy. Pediatr Surg Int 2007;23:773-8.
https://doi.org/10.1007/s00383-007-1948-0
Calinescu AM, Rougemont AL, McLin VA, Rock NM, Habre C, Wildhaber BE. A case series of prenatal hepatic hilar cyst in the presence of a gallbladder - navigating the dilemma between biliary atresia and choledochal cyst. BMC Pediatr 2024;24:580.
https://doi.org/10.1186/s12887-024-05043-z
Madadi-Sanjani O, Rohrbacher V, Uecker M. Cystic biliary atresia-a single-center, retrospective analysis. Dtsch Arztebl Int 2024;121:641-2.
https://doi.org/10.3238/arztebl.m2024.0114
Komuro H, Makino SI, Momoya T, Nishi A. Biliary atresia with extrahepatic biliary cysts-cholangiographic patterns influencing the prognosis. J Pediatr Surg 2000;35:1771-4.
https://doi.org/10.1053/jpsu.2000.19248
Suzuki T, Hashimoto T, Hussein MH, Hara F, Hibi M, Kato T. Biliary atresia type I cyst and choledochal cyst [corrected]: can we differentiate or not? J Hepatobiliary Pancreat Sci 2013;20:465-70.
https://doi.org/10.1007/s00534-013-0605-3
Chen YT, Gao MJ, Zheng ZB, Huang L, Du Q, Zhu DW, et al. Comparative analysis of cystic biliary atresia and choledochal cysts. Front Pediatr 2022;10:947876.
https://doi.org/10.3389/fped.2022.947876
Tanaka N, Ueno T, Takama Y, Fukuzawa M. Diagnosis and management of biliary cystic malformations in neonates. J Pediatr Surg 2010;45:2119-23.
https://doi.org/10.1016/j.jpedsurg.2010.06.042
Chen CJ. Clinical and operative findings of choledochal cysts in neonates and infants differ from those in older children. Asian J Surg 2003;26:213-7.
https://doi.org/10.1016/S1015-9584(09)60306-7
Ho IG, Ihn K, Jeon HJ, Lee DE, Han SJ. Optimal timing of surgery for prenatally diagnosed choledochal cysts. Front Pediatr 2023;11:1308667.
https://doi.org/10.3389/fped.2023.1308667
Caponcelli E, Knisely AS, Davenport M. Cystic biliary atresia: an etiologic and prognostic subgroup. J Pediatr Surg 2008;43:1619-24.
https://doi.org/10.1016/j.jpedsurg.2007.12.058
Davenport M, Caponcelli E, Livesey E, Hadzic N, Howard E. Surgical outcome in biliary atresia: etiology affects the influence of age at surgery. Ann Surg 2008;247:694-8.
https://doi.org/10.1097/SLA.0b013e3181638627
Hoshino E, Muto Y, Sakai K, Shimohata N, Urayama KY, Suzuki M. Age at surgery and native liver survival in biliary atresia: a systematic review and meta-analysis. Eur J Pediatr 2023;182:2693-704.
https://doi.org/10.1007/s00431-023-04925-1
Nio M, Ohi R, Miyano T, Saeki M, Shiraki K, Tanaka K. Five- and 10-year survival rates after surgery for biliary atresia: a report from the Japanese Biliary Atresia Registry. J Pediatr Surg 2003;38:997-1000.
https://doi.org/10.1016/S0022-3468(03)00178-7
Wang X, Qin Q, Lou Y. A retrospective study between type I cystic biliary atresia and infantile choledochal cyst at a tertiary centre. HK J Paediatr (new series) 2014;19:175-80.
Zhou LY, Guan BY, Li L, Xu ZF, Dai CP, Wang W, et al. Objective differential characteristics of cystic biliary atresia and choledochal cysts in neonates and young infants: sonographic findings. J Ultrasound Med 2012;31:833-41.
https://doi.org/10.7863/jum.2012.31.6.833
Nio M, Sano N, Ishii T, Sasaki H, Hayashi Y, Ohi R. Long-term outcome in type I biliary atresia. J Pediatr Surg 2006;41:1973-5.
https://doi.org/10.1016/j.jpedsurg.2006.08.019
Sasaki H, Nio M, Ando H, Kitagawa H, Kubota M, Suzuki T, et al. Anatomical patterns of biliary atresia including hepatic radicles at the porta hepatis influence short- and long-term prognoses. J Hepatobiliary Pancreat Sci 2021;28:931-41.
https://doi.org/10.1002/jhbp.989
Choungboonsri C, Sutthatarn P, Nonthasoot B, Sirichindakul B, Taesombat W, Sutherasan M, et al. Does Kasai operation prior to liver transplantation affect peri-operative outcomes in children with biliary atresia? Chula Med J 2021;65:45-9.
https://doi.org/10.58837/CHULA.CMJ.65.1.7
Vejchapipat P, Passakonnirin R, Sookpotarom P, Chittmittrapap S, Poovorawan Y. High-dose steroids do not improve early outcome in biliary atresia. J Pediatr Surg 2007;42:2102-5.
https://doi.org/10.1016/j.jpedsurg.2007.08.038
Chusilp S, Sookpotarom P, Tepmalai K, Rajatapiti P, Chongsrisawat V, Poovorawan Y, et al. Prognostic values of serum bilirubin at 7th day post-Kasai for survival with native livers in patients with biliary atresia. Pediatr Surg Int 2016;32:927-31.
https://doi.org/10.1007/s00383-016-3951-9
Sookpotarom P, Vejchapipat P, Chittmittrapap S, Chongsrisawat V, Chandrakamol B, Poovorawan Y. Short-term results of Kasai operation for biliary atresia: experience from one institution. Asian J Surg 2006;29:188-92.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Chulalongkorn Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.




