
อุบัติการณ์ ปัจจัยเสี่ยง และผลลัพธ์ทางคลินิกของการติดเชื้อแบคทีเรียแกรมลบดื้อยาหลายขนานในกระแสเลือดของโรงพยาบาลบ้านโป่ง
คำสำคัญ:
แบคทีเรียแกรมลบดื้อยาหลายขนาน, การติดเชื้อในกระแสเลือด, ปัจจัยเสี่ยง, ผลลัพธ์ทางคลินิกบทคัดย่อ
ที่มาของปัญหา: เชื้อแบคทีเรียแกรมลบดื้อยาหลายขนานในกระแสเลือด (multidrug-resistance gram-negative bloodstream infection: MDR GN-BSI) ทวีความรุนแรงขึ้นทั่วโลก นำไปสู่ข้อจำกัดในการรักษา อัตราการเสียชีวิตที่สูงขึ้น และภาระทางเศรษฐกิจอย่างก้าวกระโดด แต่ข้อมูลของโรงพยาบาลบ้านโป่งยังคงมีอยู่อย่างจำกัด
วัตถุประสงค์: เพื่อศึกษาอุบัติการณ์ ปัจจัยเสี่ยง และผลลัพธ์ทางคลินิกของการติดเชื้อแบคทีเรียแกรมลบดื้อยาหลายขนานในกระแสเลือด ณ โรงพยาบาลบ้านโป่ง จังหวัดราชบุรี
วิธีการศึกษา: การศึกษาเชิงวิเคราะห์ย้อนหลัง (retrospective analytical study) ในผู้ป่วยอายุตั้งแต่ 15 ปีขึ้นไป ที่ตรวจพบเชื้อแบคทีเรียแกรมลบในกระแสเลือดระหว่างวันที่ 1 กรกฎาคม 2566 ถึง 30 มิถุนายน 2568 โดยจำแนกกลุ่มตัวอย่างเป็นกลุ่ม MDR และ Non-MDR ตามนิยามมาตรฐานสากล เพื่อวิเคราะห์อุบัติการณ์ ปัจจัยเสี่ยง และผลลัพธ์ทางคลินิก
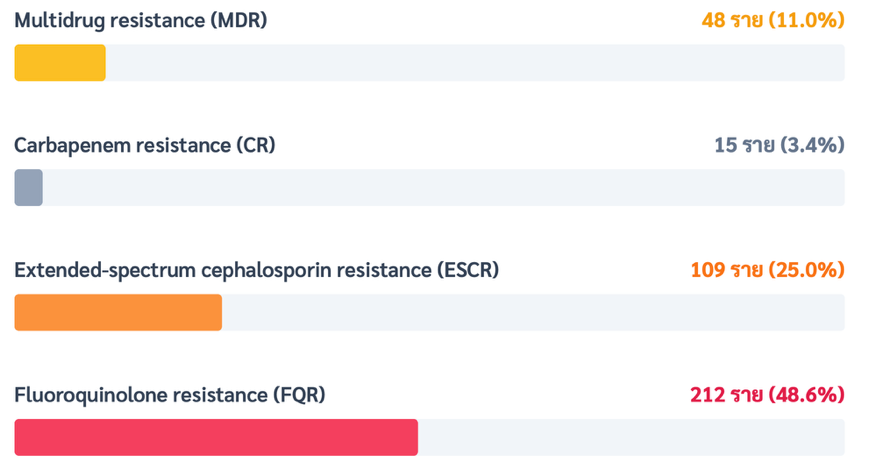
ผลการศึกษา: จากกลุ่มตัวอย่างทั้งหมด 436 ราย พบอุบัติการณ์ MDR GN-BSI ร้อยละ 11.0 เชื้อก่อโรคที่พบมากที่สุดคือ Escherichia coli และ Klebsiella pneumoniae อย่างไรก็ตาม Acinetobacter baumannii มีสัดส่วนการดื้อยาหลายขนานที่สูงกว่าเชื้อชนิดอื่นอย่างมีนัยสำคัญทางสถิติ (ร้อยละ 16.7 เทียบกับ 1.5; p<0.001) จากการวิเคราะห์ปัจจัยเสี่ยงพบว่า ปัจจัยที่มีความสัมพันธ์กับการติดเชื้อ MDR อย่างมีนัยสำคัญ ได้แก่ การติดเชื้อในโรงพยาบาล (adjusted odds ratio [aOR] 4.50, 95% confidence interval [CI] 1.25-16.20, p=0.02) ประวัติการได้รับยาต้านจุลชีพกลุ่ม Fluoroquinolones ภายใน 90 วัน (aOR 6.61, 95% CI 1.81-24.10, p=0.004) และประวัติการพบเชื้อดื้อยาหลายขนานภายใน 90 วัน (aOR 5.92, 95% CI 1.69-20.80, p=0.01) ในด้านผลลัพธ์ทางคลินิก พบว่ากลุ่ม MDR มีอัตราการเสียชีวิตสูงกว่ากลุ่ม Non-MDR อย่างชัดเจน (ร้อยละ 33.3 เทียบกับ 7.7; p<0.001) นอกจากนี้ยังสัมพันธ์กับการเกิดภาวะช็อคจากการติดเชื้อ (p=0.04) ระยะเวลานอนโรงพยาบาลที่นานขึ้นเฉลี่ย 3.6 วัน (p=0.01) การเพิ่มปริมาณการใช้ยาต้านจุลชีพชนิดออกฤทธิ์กว้าง (broad-spectrum antimicrobial agents) และค่ารักษาพยาบาลเฉลี่ยที่สูงขึ้นจาก 31,721 เป็น 51,502 บาทต่อราย (p=0.02)
สรุป: การติดเชื้อ MDR GN-BSI สัมพันธ์กับอัตราการตายและภาระทางเศรษฐกิจที่สูงขึ้นอย่างมีนัยสำคัญ การควบคุมการติดเชื้ออย่างเข้มงวดและการกำกับการใช้ยาต้านจุลชีพเป็นมาตรการเร่งด่วนที่จำเป็น
เอกสารอ้างอิง
World Health Organization. Global antimicrobial resistance and use surveillance system (GLASS) report 2024. Geneva: WHO; 2024.
Logan LK, Weinstein RA. The epidemiology of carbapenem-resistant enterobacteriaceae: the impact and evolution of a global menace. J Infect Dis. 2017;215(Suppl 1):S28–S36. doi: 10.1093/infdis/jiw282.
Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America 2022 guidance on the treatment of extended-spectrum β-lactamase producing enterobacterales (ESBL-E), carbapenem-resistant enterobacterales (CRE), and pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa). Clin Infect Dis. 2022;75(2):187-212. doi: 10.1093/cid/ciac268.
Magiorakos AP, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–81. doi: 10.1111/j.1469-0691.2011.03570.x.
National Antimicrobial Resistance Surveillance Center, Thailand (NARST). Antimicrobial resistance report 2023. Bangkok: NARST; 2024.
Schwaber MJ, Carmeli Y. Mortality and delay in effective therapy associated with extended-spectrum beta-lactamase production in enterobacteriaceae bacteremia: a systematic review and meta-analysis. J Antimicrob Chemother. 2007;60(5):913–20. doi: 10.1093/jac/dkm318.
Sahu C, Jain V, Singh P. Risk factors and outcomes of multidrug-resistant gram-negative infections in intensive care unit patients: a prospective observational study. Indian J Crit Care Med. 2020;24(6):420–6.
Phumart P, Phodha T, Thamlikitkul V, Riewpaiboon A, Prakongsai P, Limwattananon S. Health and economic impacts of antimicrobial resistant infections in Thailand. J Health Syst Res. 2012;6(3):352-60.
Lueangarun S, Thamlikitkul V, Tongsai S. Risk factors and outcomes of carbapenem-resistant enterobacteriaceae bloodstream infection in Thailand. J Med Assoc Thai. 2021;104(7):1010–8.
Apisarnthanarak A, Mundy LM. Epidemiology of multidrug-resistant gram-negative bacteria in Thailand. Infect Control Hosp Epidemiol. 2018;39(9):1180–3.
Soravipukuntorn T, Thammahong A, Charoenpong L, Suttha P, Manosuthi W. Outcomes and associated factors among patients with multidrug-resistant gram-negative bacilli bacteremia at a tertiary care hospital in Thailand. J Med Assoc Thai. 2025;108(1):31-40. doi: 10.35755/jmedassocthai.2025.1.30-41-01303.
Chaisathaphol T, Chayakulkeeree M. Epidemiology of infections caused by multidrug-resistant gram-negative bacteria in adult hospitalized patients at Siriraj Hospital. J Med Assoc Thai. 2014;97(Suppl 3):S35-S45.
Centers for Disease Control and Prevention (CDC). Antibiotic resistance (AR) option protocol. Atlanta (GA): CDC; 2015.
Dalhoff A. Global fluoroquinolone resistance epidemiology and implications for clinical use. Interdiscip Perspect Infect Dis. 2012;2012:976273. doi: 10.1155/2012/976273.
Weiner LM, Webb AK, Limbago B, Dudeck MA, Patel J, Kallen AJ, et al. Antimicrobial-resistant pathogens associated with healthcare-associated infections: summary of data reported to the National Healthcare Safety Network at the CDC, 2011–2014. Infect Control Hosp Epidemiol. 2016;37(11):1288–301. doi: 10.1017/ice.2016.174.
Rizzo K, Horwich-Scholefield S, Shimano KA. Carbapenem and cephalosporin resistance among Enterobacteriaceae: CDC phenotype definitions applied in clinical surveillance. Open Forum Infect Dis. 2019;6(6):ofz244.
Azerefegne EF, Tasamma AT, Demass TB, Tessema AG, Degu WA. Prevalence of multidrug resistant gram-negative bacteria and associated factors among gram-negative blood culture isolates at Tikur Anbessa Specialized Hospital: a retrospective study. BMC Infect Dis. 2025;25(1):1006. doi: 10.1186/s12879-025-11328-0.
Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399:629-55. doi: 10.1016/S0140-6736(21)02724-0.
Ponyon J, Kerdsin A, Preeprem T, Ungcharoen R. Risk factors of Infections due to multidrug-resistant gram-negative bacteria in a community hospital in rural Thailand. Trop Med Infect Dis. 2022;7:328. doi: 10.3390/tropicalmed7110328.
Porter KA, Rhodes J, Dejsirilert S, Henchaichon S, Siludjai D, Thamthitiwat S, et al. Acinetobacter bacteraemia in Thailand: evidence for infections outside the hospital setting. Epidemiol Infect. 2014;142(6):1317–27. doi: 10.1017/S0950268813002082.
Inchai J, Liwsrisakun C, Theerakittikul T, Chaiwarith R, Khositsakulchai W, Pothirat C. Risk factors of multidrug-resistant, extensively drug-resistant and pandrug-resistant acinetobacter baumannii ventilator-associated pneumonia in a Medical Intensive Care Unit of University Hospital in Thailand. J Infect Chemother. 2015;21(8):570-4. doi: 10.1016/j.jiac.2015.04.010.
Werarak P, Kiratisin P, Thamlikitkul V. Hospital-acquired pneumonia and ventilator-associated pneumonia in adults at Siriraj Hospital. J Med Assoc Thai. 2010;93 (Suppl 1):S126-S138.
Wangchinda W, Laohasakprasit K, Lerdlamyong K, Thamlikitkul V. Epidemiology of carbapenem-resistant enterobacterales infection and colonization in hospitalized patients at a university hospital in Thailand. Infect Drug Resist. 2022;15:2199–210. doi: 10.2147/IDR.S361013.
Zollner-Schwetz I, Zechner E, Ullrich E, Luxner J, Pux C, Pichler G, Schippinger W, et al. Colonization of long term care facility patients with MDR-Gram-negatives during an acinetobacter baumannii outbreak. Antimicrob Resist Infect Control. 2017;6:49. doi: 10.1186/s13756-017-0209-9.
Yassin A, Huralska M, Pogue JM, Dixit D, Sawyer RG, Kaye KS. State of the management of infections caused by multidrug-resistant gram-negative organisms. Clin Infect Dis. 2023;77(9):e46–e56. doi: 10.1093/cid/ciad499.
Lim C, Hantrakun V, Klaytong P, Rangsiwutisak C, Tangwangvivat R, Phiancharoen C, et al. Higher frequency and mortality rate following antimicrobial-resistant bloodstream infections in tertiary-care hospitals compared with secondary-care hospitals in Thailand. medRxiv [Preprint]. 2023:2023.02.07.23285611. doi: 10.1101/2023.02.07.23285611.
European Centre for Disease Prevention and Control. Carbapenem-resistant enterobacterales: third update. Stockholm: ECDC; 2025.
Phodha T, Riewpaiboon A, Malathum K, Coyte PC. Excess annual economic burdens from nosocomial infections caused by multi-drug resistant bacteria in Thailand. Expert Rev Pharmacoecon Outcomes Res. 2019;19(3):305-12. doi: 10.1080/14737167.2019.1537123.
Rattanaumpawan P, Choorat C, Takonkitsakul K, Tangkoskul T, Seenama C, Thamlikitkul V. A prospective surveillance study for multidrug-resistant bacteria colonization in hospitalized patients at a Thai University Hospital. Antimicrob Resist Infect Control. 2018;7:102. doi: 10.1186/s13756-018-0393-2.
Capsoni N, Bellone P, Aliberti S, Sotgiu G, Pavanello D, Visintin B, et al. Prevalence, risk factors and outcomes of patients coming from the community with sepsis due to multidrug resistant bacteria. Multidiscip Respir Med. 2019;14:23. doi: 10.1186/s40248-019-0185-4.
ดาวน์โหลด
เผยแพร่แล้ว
รูปแบบการอ้างอิง
ฉบับ
ประเภทบทความ
สัญญาอนุญาต
ลิขสิทธิ์ (c) 2026 ราชภิวัฒน์เวชสาร

อนุญาตภายใต้เงื่อนไข Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Articles in this journal are copyrighted by the x may be read and used for academic purposes, such as teaching, research, or citation, with proper credit given to the author and the journal.use or modification of the articles is prohibited without permission.
statements expressed in the articles are solely the opinions of the authors.
authors are fully responsible for the content and accuracy of their articles.
other reuse or republication requires permission from the journal."

