
Clinical factors predicting the need for biopsy in children with cervical lymphadenopathy
Keywords:
Cervical lymphadenopathy, children, granulomatous lymphadenitis, lymphoma, reactive lymphoid hyperplasiaAbstract
Background: Diagnosing lymphadenopathy in children can be challenging for clinicians, as it may represent a manifestation of various conditions, including granulomatous diseases and malignancies. The cervical region is frequently affected in cases of peripheral lymphadenopathy. While surgical biopsy can provide a definitive diagnosis, it is not always necessary.
Objectives: This study aimed to characterize pediatric patients with cervical lymphadenopathy who underwent surgical biopsy and to identify clinical factors associated with lymph nodes that require further management (LNFM), such as those with granulomatous or malignant features.
Methods: A retrospective review was conducted on 87 pediatric cases of cervical lymphadenopathy that underwent surgical biopsy. A descriptive analysis was performed. Receiver operating characteristic (ROC) analysis was used to identify the lymph node size most indicative of LNFM. Logistic regression analysis was conducted to determine independent predictors of LNFM, granulomatous lymph nodes, and malignant lymph nodes.
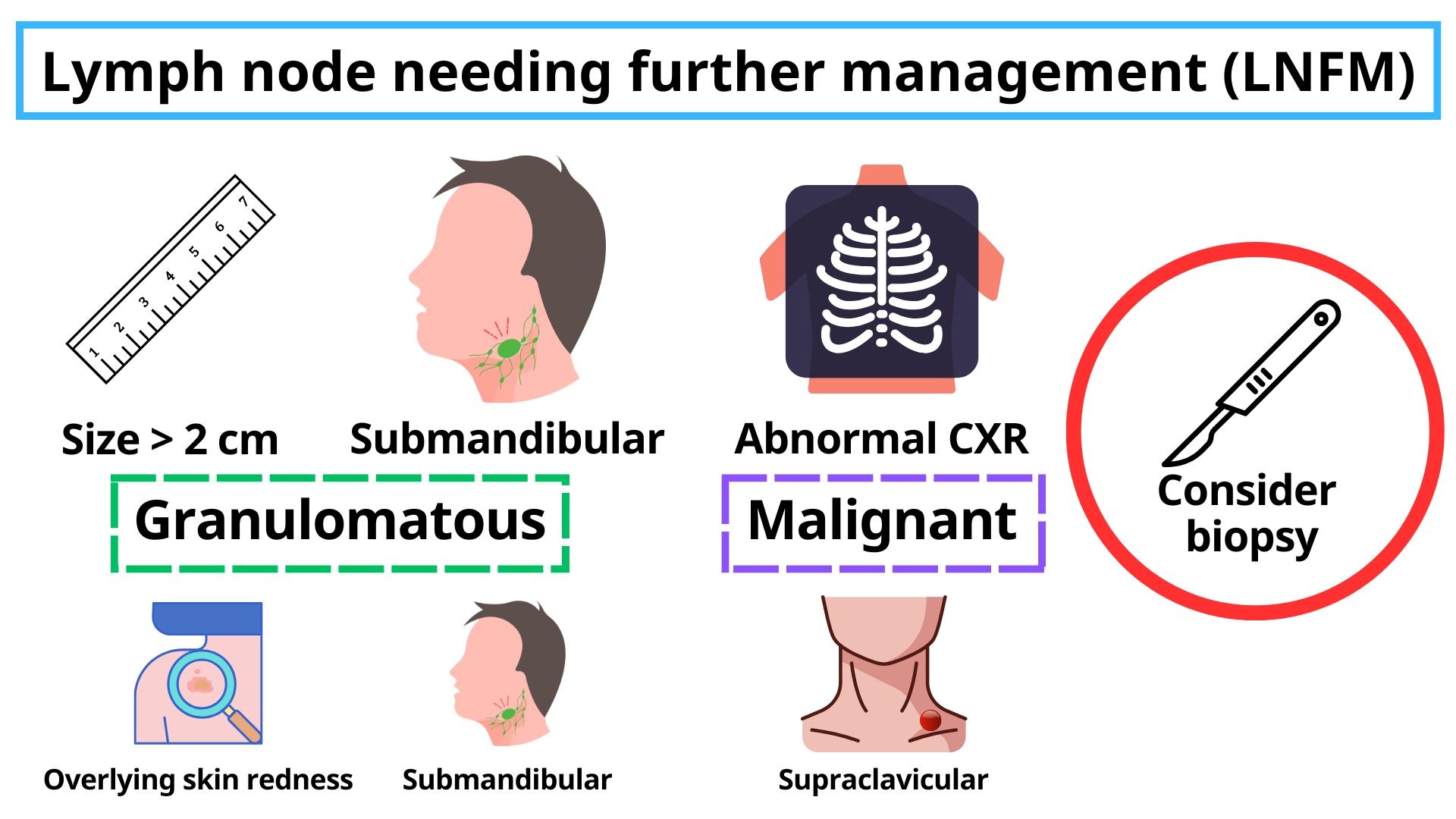
Results: Final diagnoses revealed 37 cases (42.5%) as non-LNFM, 36 cases (41.4%) as granulomatous, and 14 cases (16.1%) as malignant lymph nodes. ROC analysis identified 2 cm as the optimal lymph node size threshold for predicting LNFM, balancing sensitivity and specificity. Multivariate logistic regression revealed that submandibular location (overlying skin redness (OR), 11.9; 95% confidence intervals (CI), 2.5–55.4; P = 0.002) and abnormal chest x-ray findings (OR, 20.7; 95% CI, 2.1–201.5; P = 0.009) were independent predictors of LNFM. Subgroup analysis further showed that OR, 8.0; 95% CI, 1.1–58.8; P = 0.04) and submandibular location (OR, 9.7; 95% CI, 1.3–72.1; P = 0.027) were significant predictors of granulomatous lymph nodes. No significant predictors were found for malignant lymph nodes.
Conclusion: Submandibular location and abnormal chest x-ray findings serve as key predictors of LNFM. Lymph nodes exceeding 2 cm in size are more likely to fall into the LNFM category. OR and submandibular involvement suggest granulomatous pathology. Most supraclavicular nodes were classified as LNFM and were frequently malignant, underscoring the need for careful assessment of this area. These findings may support clinical decision-making prior to biopsy in cases of cervical lymphadenopathy.
Downloads
References
Grant CN, Aldrink J, Lautz TB, Tracy ET, Rhee DS, Baertschiger RM, et al. Lymphadenopathy in children: a streamlined approach for the surgeon - a report from the APSA Cancer Committee. J Pediatr Surg 2021; 56:274 81.
https://doi.org/10.1016/j.jpedsurg.2020.09.058
Freeman AM, Matto P. Lymphadenopathy. In:StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025.
Weinstock MS, Patel NA, Smith LP. Pediatric cervical lymphadenopathy. Pediatr Rev 2018;39:433 43.
https://doi.org/10.1542/pir.2017-0249
Moore SW, Schneider JW, Schaaf HS. Diagnostic aspects of cervical lymphadenopathy in children in the developing world: a study of 1,877 surgical specimens. Pediatr Surg Int 2003;19:240 4.
https://doi.org/10.1007/s00383-002-0771-x
Gallois Y, Cogo H, Debuisson C, Guet-Revillet H, Brehin C, Baladi B, et al. Nontuberculous lymphadenitis in children: What management strategy? Int J Pediatr Otorhinolaryngol 2019;122:196 202.
https://doi.org/10.1016/j.ijporl.2019.04.012
Meoli A, Deolmi M, Iannarella R, Esposito S. Nontuberculous mycobacterial diseases in children. Pathogens 2020;9:553.
https://doi.org/10.3390/pathogens9070553
Farndon S, Behjati S, Jonas N, Messahel B. How to use… lymph node biopsy in paediatrics. Arch Dis Child Educ Pract Ed 2017;102:244 8.
https://doi.org/10.1136/archdischild-2015-309634
Deosthali A, Donches K, DelVecchio M, Aronoff S. Etiologies of pediatric cervical lymphadenopathy: a systematic review of 2687 subjects. Glob Pediatr Health 2019;6:2333794X19865440.
https://doi.org/10.1177/2333794X19865440
Absalon MJ, Khoury RA, Phillips CL. Post-transplant lymphoproliferative disorder after solid-organ transplant in children. Semin Pediatr Surg 2017; 26:257 66.
https://doi.org/10.1053/j.sempedsurg.2017.07.002
Bozlak S, Varkal MA, Yildiz I, Toprak S, Karaman S, Erol OB, et al. Cervical lymphadenopathies in children: A prospective clinical cohort study. Int J Pediatr Otorhinolaryngol 2016;82:81 7.
https://doi.org/10.1016/j.ijporl.2016.01.002
Celenk F, Gulsen S, Baysal E, Aytac I, Kul S, Kanlikama M. Predictive factors for malignancy in patients with persistent cervical lymphadenopathy. Eur Arch Otorhinolaryngol 2016;273:251 6.
https://doi.org/10.1007/s00405-015-3717-3
Wang J, Pei G, Yan J, Zhao Q, Li Z, Cao Y, et al. Unexplained cervical lymphadenopathy in children: predictive factors for malignancy. J Pediatr Surg 2010;45:784 8.
https://doi.org/10.1016/j.jpedsurg.2009.08.018
Indolfi P, Perrotta S, Rossi F, Di Martino M, Pota E, Di Pinto D, et al. Childhood Head and Neck Lymphadenopathy: A report by a Single Institution (2003-2017). J Pediatr Hematol Oncol 2019;41:17 20.
https://doi.org/10.1097/MPH.0000000000001273
Shah I, Dani S. Profile of Tuberculous cervical lymphadenopathy in children. J Trop Pediatr 2017;63:395 8.
https://doi.org/10.1093/tropej/fmx001
Loizos A, Soteriades ES, Pieridou D, Koliou MG. Lymphadenitis by non-tuberculous mycobacteria in children. Pediatr Int 2018;60:1062 7.
https://doi.org/10.1111/ped.13708
Garcia-Marcos PW, Plaza-Fornieles M, Menasalvas-Ruiz A, Ruiz-Pruneda R, ParedesReyes P, Miguelez SA. Risk factors of nontuberculous mycobacterial lymphadenitis in children: a case-control study. Eur J Pediatr 2017;176:607 13.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 Chulalongkorn Medical Journal

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.




