
Factors associated with 28-day readmission among patients with chronic obstructive pulmonary disease, Cha-uat Hospital, Nakhon Si Thammarat Province
Keywords:
Patients, 28-day Readmission, Chronic Obstructive Pulmonary DiseaseAbstract
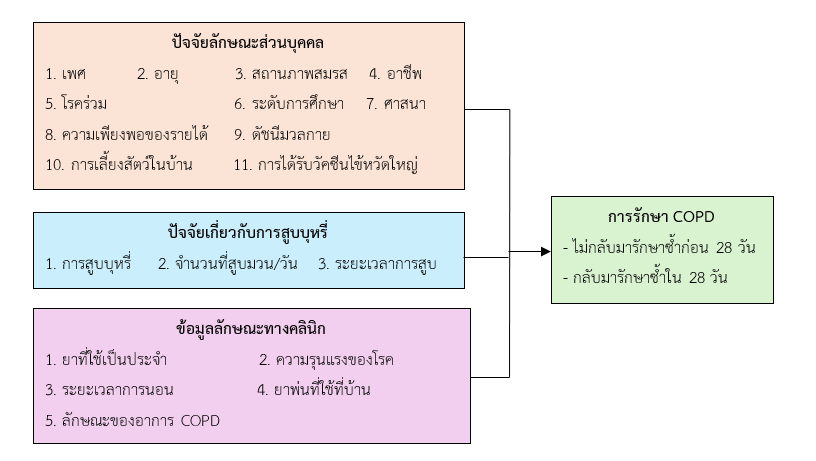
This retrospective analytical study aimed to examine factors associated with 28-day readmission among patients with chronic obstructive pulmonary disease (COPD), Cha-uat Hospital, Nakhon Si Thammarat Province. The population consisted of patients treated for COPD, who were divided into two groups: 73 patients who were not readmitted and 189 patients who were readmitted within 28 days. The research instrument was data from medical records. Content validity was assessed by three experts with an Item-Objective Congruence (IOC) index of 1.00 for all items. Data were analyzed using descriptive statistics and multivariable logistic regression.
The results showed that factors associated with 28-day readmission among COPD patients included the following: female patients had a higher likelihood of readmission compared with male patients (adj.OR = 175.70, 95% CI = 15.71–1,964.57). Patients aged 60–69 years and 70–79 years had a lower likelihood of readmission compared with those aged ≤59 years (adj.OR = 0.001, 95% CI = 0.01–0.10 and adj.OR = 0.001, 95% CI = 0.01–0.05, respectively). Patients with general labor occupations had a lower likelihood of readmission (adj.OR = 0.02, 95% CI = 0.01–0.40), whereas those who were traders or homemakers had a higher likelihood of readmission compared with those engaged in agriculture (adj.OR = 61.45, 95% CI = 2.64–1,430.13 and adj.OR = 77.62, 95% CI = 3.56–1,692.45, respectively). Patients with an education level higher than primary school had a lower likelihood of readmission compared with those with primary education (adj.OR = 0.06, 95% CI = 0.01–0.66). Patients with insufficient income relative to expenses had a higher likelihood of readmission compared with those whose income was sufficient (adj.OR = 22.02, 95% CI = 2.89–167.57). Smokers had a significantly higher likelihood of readmission compared with non-smokers (adj.OR = 26,553.57, 95% CI = 501.25–1,406,663.59). Patients with severe disease classified as GOLD C–D had a higher likelihood of readmission compared with those classified as GOLD A–B (adj.OR = 131.59, 95% CI = 10.44–1,658.05). In addition, patients with a hospital length of stay of ≥8 days had a higher likelihood of readmission compared with those with a length of stay of 1–7 days (adj.OR = 753.53, 95% CI = 9.98–56,904.06).
Therefore, professional nurses should develop behavior modification programs targeting risk factors associated with COPD exacerbation and readmission. Such programs should emphasize increased involvement of family members to enhance awareness of the severity of COPD exacerbations and to support patients in preventing recurrent episodes.
References
กนกวรรณ อนุศักดิ์, รัตนนุช มาธนะสารวุฒิ, โภคิน ศักรินทร์กุล, & วิชุดา จิรพรเจริญ. (2564). ปัจจัยที่มีความสัมพันธ์ต่อการเกิดอาการกำเริบเฉียบพลันในผู้ป่วยโรคปอดอุดกั้นเรื้อรังที่มารับการรักษาที่ห้องฉุกเฉินโรงพยาบาลลำพูน. วารสารกรมการแพทย์, 46(4), 67–73.
กระทรวงสาธารณสุข. (2566). อัตราป่วยรายใหม่ของโรคปอดอุดกั้นเรื้อรัง.
กระทรวงสาธารณสุข. (2567). ตัวชี้วัด Service plan ปี 2567.
ชมขวัญ แก้วพลงาม, ณัฐวดี อินทเเสน, ภานุพงษ์ อุ่นเรือนงาม, & ปาริชาติ นิยมทอง. (2565). ปัจจัยพยากรณ์ที่มีความสัมพันธ์ต่อการเกิดภาวะกำเริบเฉียบพลันในผู้ป่วยโรคปอดอุดกั้นเรื้อรัง. วารสารสาธารณสุขแพร่เพื่อการพัฒนา, 30(1), 99–111.
ธนิตดา เลิศลอยกุลชัย. (2563). ปัจจัยทางคลินิกของผู้ป่วยโรคปอดอุดกั้นเรื้อรังที่ต้องนอนโรงพยาบาลซ้ำใน 28 วัน เนื่องจากภาวะกำเริบเฉียบพลันในโรงพยาบาลสมเด็จพระพุทธเลิศหล้า. วารสารแพทย์เขต 4-5, 39(2), 37–48.
โรงพยาบาลชะอวด. (2567). รายงานผู้ป่วยโรคปอดอุดกั้นเรื้อรัง. สำนักงานสาธารณสุขจังหวัดนครศรีธรรมราช.
วิชิต ธีรไกรศรี. (2567). ปัจจัยที่มีความสัมพันธ์ต่อการกำเริบเฉียบพลันของผู้ป่วยโรคปอดอุดกั้นเรื้อรังในโรงพยาบาลพหลพลพยุหเสนา จังหวัดกาญจนบุรี. วารสารโรงพยาบาลพหลพลพยุหเสนา, 13(1), 57–69.
ศุภนิดา คำนิยม. (2567). ปัจจัยที่สัมพันธ์กับการเกิดภาวะกำเริบเฉียบพลันของผู้ป่วยโรคปอดอุดกั้นเรื้อรังที่นอนโรงพยาบาลซ้ำใน 28 วัน: โรงพยาบาลยโสธร. ยโสธรเวชสาร, 26(1), 108.
ศูนย์วิจัยและจัดการความรู้เพื่อการควบคุมยาสูบ. (2557). สรุปสถานการณ์ปัจจัยเสี่ยงหลักด้านยาสูบของประเทศไทย พ.ศ. 2557. มหาวิทยาลัยมหิดล.
สมคิด ขำทอง, ปิ่นหทัย ศุภเมธาพร, & ยุวยงค์ จันทรพิจิตร. (2562). ปัจจัยทำนายการเกิดอาการกำเริบเฉียบพลันในผู้ป่วยโรคปอดอุดกั้นเรื้อรัง. พยาบาลสาร, 46(1), 126–136.
สมาคมอุรเวชช์แห่งประเทศไทยในพระบรมราชูปถัมภ์. (2560). ข้อแนะนำการดูแลรักษาผู้ป่วยโรคปอดอุดกั้นเรื้อรัง พ.ศ. 2560.
สำนักงานสาธารณสุขจังหวัดนครศรีธรรมราช. (2567). ข้อมูลรายงานผู้ป่วยโรคปอดอุดกั้นเรื้อรัง. กระทรวงสาธารณสุข.
สุภาพร ณ พัทลุง. (2567). ความชุกและปัจจัยที่มีความสัมพันธ์ต่อการกลับมารักษาซ้ำใน 28 วัน ของผู้ป่วยโรคปอดอุดกั้นเรื้อรัง โรงพยาบาลสิงหนคร. วารสารนวัตกรรมสุขภาพและความปลอดภัย, 1(2), 24–34.
อุษา เอี่ยมละออ, เยาวเรศ สายสว่าง, ปิยะลักษณ์ ฉายสุวรรณ, & อารีย์ โกพัฒนกิจ. (2561). อุบัติการณ์และปัจจัยเสี่ยงต่อการกลับมารักษาซ้ำใน 28 วัน ของผู้ป่วยโรคปอดอุดกั้นเรื้อรัง ในโรงพยาบาลอ่างทอง. วารสารวิชาการมหาวิทยาลัยอีสเทิร์นเอเชีย ฉบับวิทยาศาสตร์และเทคโนโลยี, 12(2), 240–252.
Global Initiative for Chronic Obstructive Lung Disease. (2021). The global strategy for the diagnosis, management and prevention of COPD. http://www.goldcopd.org
Mannion, D. M., Homa, D. M., Akinbami, L. J., Ford, E. S., & Redd, S. C. (2002). Chronic obstructive pulmonary disease surveillance—United States, 1971–2000. MMWR Surveill Summ, 51(6), 1–16.
Milne, K. M., Mitchell, R. A., Ferguson, O. L., Hind, A. S., & Guenette, J. A. (2024). Sex-differences in COPD: From biological mechanisms to therapeutic considerations. Frontiers in Medicine, 20(11), Article 1289259. https://doi.org/10.3389/fmed.2024.1289259
Tombor, I., Vangeli, E., West, R., & Shahab, L. (2017). Progression towards smoking cessation: Qualitative analysis of successful, unsuccessful, and never quitters. Journal of Substance Use, 23(2), 214–222. https://doi.org/10.1080/14659891.2017.1378746
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Journal of Primary Health Research

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.




